Disclaimer: My infographic was a result of ChatGPT replying to a line of inquiry I made about generic drug manufacturing AND combined it with what some economic and policy wonks define as what they consider “fair pricing”.
As you read my article, it appears the current global generic medication manufacturing industry is presently experiencing profit margins above the “fair” category. Patented drug manufacturing makes evan wider margins of profit and this takes into account the massive spend on advertising AND the less massive spend on research and development. Armed with this information, I think government policy for pharma definitely needs revision and the Trump administration’s announcement to address US drug prices is a correct priority. Likewise hospital payment and health insurance reform is WAY PAST DUE.

Awhile back, I wrote a lengthy post about the Glp-agonist drug class and how MARKETS WILL BE MADE. It was titled Good God Almighty Which Way Do I Steer?
Interestingly my “armchair” analysis concluded that the market price for the sweet spot of the “perception of affordability” for this revolutionary drug class was between $150-300 a month. As the big pharma boys line up for this market, it is interesting to note that they are falling over themselves to provide cash price access for single vial delivery about 200% above my guesstimate. Could this be construed as price fixing?
Novo Nordisk’s Wegovy initial month cash offer is $199 and $499 thereafter. Lilly’s Zepbound has a convoluted offer of discounting pricing scheme if you try insurance and get denied. They cap your out of pocket discounts to between $3-6 thousand depending upon your crappy plan. They also offer a cash price of the single vial doses at $499. Hint: Just bypass your insurance offer unless “covered” (you never are) as the better individual cost is to go with the cash price offer.
From my prior Glp agonist review post, regarding what people will afford for effective weight loss medication, the following quote is referenced.
Of all the ones that hit the market and worked the best, Vivus’s Qsymia was marketed at a price people find appropriate. This is my go-to prescription for weight loss because we can get the real drug through a specialty mail-order pharmacy. The pharmacy is contracted by the manufacturer to provide a cash price right at 100 dollars a month. This folks is the cash market!
Regarding Qsymia and other patented weight loss products, I noted that going significantly above 100 dollars a month pretty much was a deal breaker for a chronic weight loss medication. I did learn in my research for this article that Vivus got patent extension through 2029. It was doing to run out in 2020- I don’t know why the FDA extended it.
As compounded, I am learning from patients that semaglutide is available from 150-350 dollars a month and they are paying this willingly. The name brand Ozempic is retailing above 1000 bucks a month. To me it seems Big Pharma is like Big Hospital -they command at least 10 times the market price for their services. This is why the myth that health insurance is necessary for health care continues.
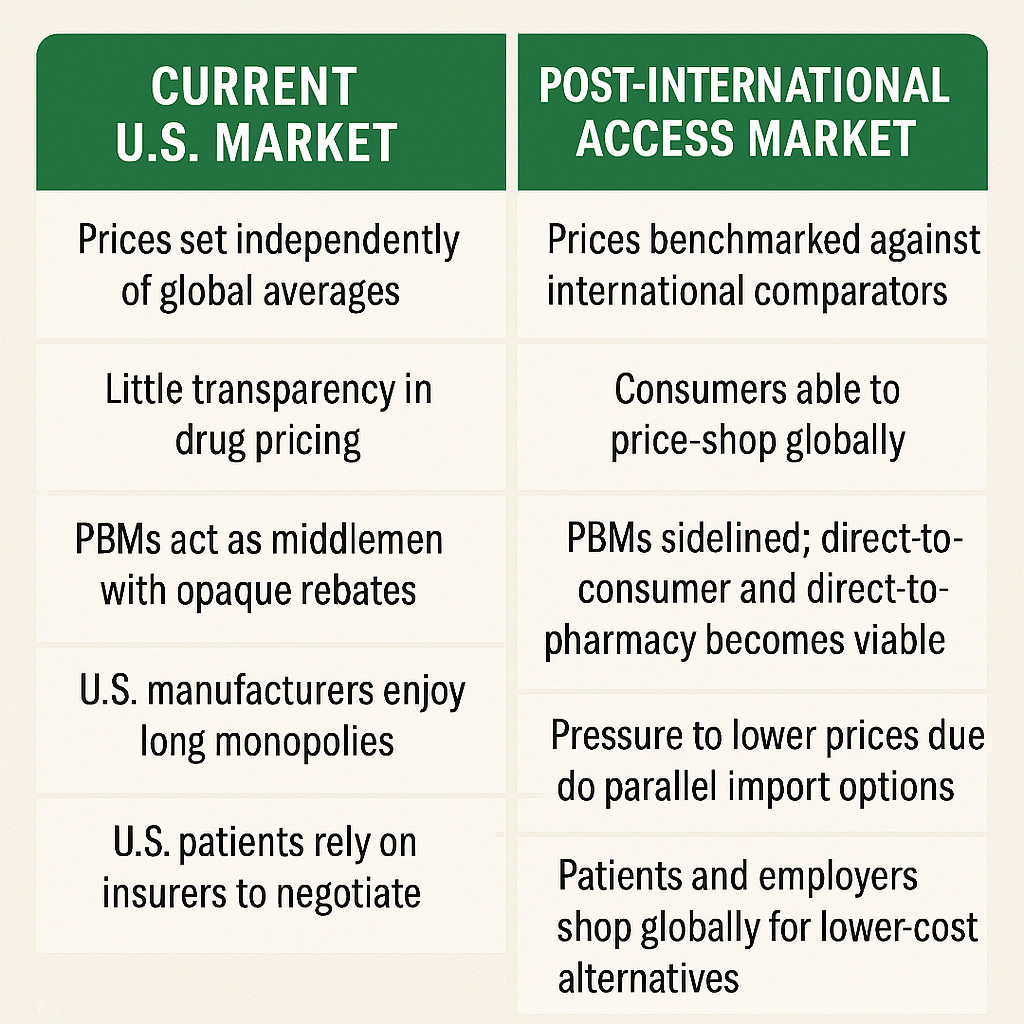
My last post covered the history of pharmaceutical patents and was an attempt to expose the fact that United States market regulation of big pharma is why we pay the lion’s share of global prescription drug costs (and profits).
What Is The Industry Doing For Damage Control Regarding The Trump Administration’s Plan for “Delivering Most-Favored-Nation Prescription Drug Pricing to American Patients.”

This week in the news, the large Swiss generic manufacturer Sandoz’s CEO, Richard Saynor, has been publicly discussing tariffs on generic drug imports and their impact on U.S. markets:
He claims that potential tariff mischief will be counter productive to US generic manufacturing incentives. He is asking for policy to “incentivize” manufacturing to cross the ocean and into the United States.
Mr. Saynor warns:
Tariffs will lead to supply disruptions and higher costs to individuals.
Saynor warns that imposing tariffs—or even threatening them—discourages generics manufacturers from investing in U.S. production capacity.
He points out generics operate on thin margins, producing essential medicines like antibiotics for less than the cost of everyday items.
He claims U.S. plants cost $2–3 billion each and without government incentives, tariffs won’t prompt investment.
Does it really cost $2-3 billion to get in the generics game?
I took a deeper dive into this question and I also explored what kind of manufacturing capacity and options presently exist in the market. The answer appears that his claims are credible IF you are looking at a full-on biologics manufacturing model with full regulatory compliance and scale for sustainable manufacturing. Recall in my most recent post I discussed how the US legal regulatory policy is promoting and protecting biologicals as the go to most profitable and protective route for pharmaceutical innovation to take.
On the other hand if you look at starting up a generic oral pill chemical drug you are looking at 10’s of millions to a billion dollars for the full on project. You can start a small lab and production facility for 100’s to a few million.

I asked ChatGPT for a summary of generic manufacturing capacity and head counts. Here is the summary:
Global top 15: A mix of U.S., Indian, Israeli, Swiss, and Japanese generics firms.
U.S. Top Players: Viatris, Abbott, AbbVie, Amneal, Teva USA.
Total U.S. Generics Facilities: ~600–700 registered manufacturing sites, representing a vibrant domestic generics ecosystem.
Yes — there is manufacturing capacity and competition in the U.S., especially in generics and biotech. Further there is a massive global manufacturing capacity. So why then can’t the market deliver chronic-use, brand-name drugs affordably to U.S. and global consumers? The top 15 manufacturers together account for a major share of global generic revenue (~$400+ billion market).
Here is a little side note: If it takes 2 billion to build a new full on manufacturing facility and noting the sales dollars we are looking at new plant cost to annual revenues of 0.5%
Mr. Saynor points out that the generic drug manufacturing business is a low margin business. I asked ChatGPT how economists and businesses define profit margins from low to high profit margins:
How Profit Margins Are Classified by Industry
🔹 Net Profit Margin (after all costs, including taxes)

It appears from benchmark information it is not a true statement that generic medication production is a low margin business. It is in fact a moderate margin business. Mr. Saynor appears incorrect on that claim.
It also is obvious that we don’t have an inadequate supply chain for generic medication manufacturing. Will tariffs directed at non US production disincentivize market participation? Surely, given using other countries for manufacturing allows generic drug production to be a moderate margin business. Will tariffs on global generic manufacturing result in more US production? I think what Mr. Sandor is telling us is “no” BUT if we give him and the global generic medication industry subsidies (perhap from the tariff revenue), he could find the motivation to move more jobs our way.
What Could Big Pharma Do To Help Its Customers?
An obvious pivot for long term survival and to get in front of what might be inevitable unfavorable future federal regulation, is to consider providing their name brand product as an ongoing market option AFTER the patent expires. This doesn’t happen now and the reason is IF they moved to competitive generic price competition for their name brand, government could come after them for what is obviously price gouging/predatory pricing that is currently in place. Maybe the pharma lobbies congress for a mea culpa on the past price gouging for protection to move to this business model? Just a thought (and not a bad one I might add).
I would submit that had Merck kept the Zocor brand name and offered it as a generic competitor price 10-20% higher than the white labeled generics “settled” market price, they would have maintained a large market share AND continue to make a moderate or more than moderate profit margin- indefinitely. Over the counter Tylenol is a perfect example of what I am talking about. When you go from 10 dollars a pill to 30 cents a pill to stick with the brand name, I suspect many buyers would chose the brand name.
Big pharma should offer price caps on personal out of pocket payment for chronic medication products. It isn’t reasonable to ask any individual to pay for one medication on an annual basis which cost is higher than their grocery bill. Given the present extended duration of patent protection currently enjoyed, and noting my prior documentation that pharma gets their return on investment in 3-4 years, there appears to be plenty of fat there to consider this type of policy. If you can’t get something into the market for less than a person’s annual grocery bill, perhaps you should move onto a different project. We can’t keep paying ever rising and frankly ridiculous extorted prices, made possible by federal regulatory favoritism to pharma, especially acknowledging that 90% of present medication use is in the generic world COMBINED with the understanding that generic medication manufacturing is presently a moderate to high moderate profit industry.