


A Recent Shingrix Vaccine Study Provides Useful Information on Efficacy
A Recent Shingrix Vaccine Study Provides Useful Information on Efficacy
And Commentary On An Editorial Discussing Physician Unions

We aren’t talking about this kind of shingles.
The doctor lay-term for acute herpes zoster is called “shingles”. This is a painful recurrence of childhood chicken pox. Chicken pox results from infection of a virus named varicella virus. It is a member of the herpes virus family.
For some reason, humans have a penchant for hosting the herpes family of viruses AND an insufficient immune system for getting rid of this group of virions. Examples include oral and genital herpes. Both of these common symptomatic illnesses tend to be recurrent in a significant portion of people. Herpes 1 and 2 are the pathogens for oral and genital herpes, respectfully. Clinically, herpes 1 (mostly) virus can infect the brain resulting in acute herpes encephalitis. This form of brain infection presents as altered mental status and is associated with significant mortality. MRI shows classic findings to help make this diagnosis. It responds to antiviral therapy and so it is important to recognize and diagnose. Herpes one and two are amenable to antiviral therapy as well. If people have several recurrences we can prescribe daily dosing to prevent clinical outbreaks. This works.
I personally have diagnosed a varicella encephalitis in an elderly female (pre vaccine era). She presented with a severely painful throat. The clue was the syndrome didn’t respond to oral antibiotics AND her symptoms were confined to one side of her pharynx/throat. On repeat examination, I found vesicles (that is a feature of the classic shingles rash) in her left ear canal and along her left upper palate. She developed altered mental status and fevers as I initiated treatment. She was hospitalized and placed on IV acyclovir and thankfully fully recovered.
I am mentioning this particular case to illustrate that these syndromes can become very serious especially in immunocompromised and older patients.
In the case of shingles, the sensory ganglion of the spinal cord is the “jail cell” where dormant varicella virus is harbored. For various reasons, the virus can escape immune surveillance and replicate sufficiently to initiate active infection and symptoms. It often starts with sensory pain. As the virus migrates up and out the sensory nerve dermatome, the pain localizes along the involved nerve roots. Patients can present to the doctor with burning and intense pain with no initial physical findings. As the virus follows the nerve root to the most distal and small fibers, it manifests in the skin as a red based blistering and weeping rash. The blisters are teeming with active replicating virus. Early recognition and treatment with antiviral medication can significantly improve the worse-case outcome of persistent permanent noxious pain even after the rash resolves. Patients have become opioid dependent and permanently disabled from the shingle neuralgia that can follow.
As explained above, shingles/herpes zoster results from a tissue escape of dormant varicella virus. The theory is the virus lies in waiting in the sensory ganglia of the spinal nervous system predominantly. It can involve the cranial nerve roots as well. The cranial nerves are important large nerve roots arising from the brainstem (skull compartment) and innervate the eye, hearing, face, tongue, and the first cranial nerve is responsible for the sense of smell (olfactory nerve). Patients can get eye involvement of shingles. This can result in tissue injury and permanent visual loss, not to mention the horrible pain associated with shingles.
Noting the morbidity and high incidence of clinical shingles in adults, it made sense to seek a way to prevent the condition. Vaccination has been shown to work in lowering the rate of clinical adult shingles. It isn’t perfect and the long term experience with the original varicella adult vaccine left room for improvement. Enter the Shingrix (recombinant zoster vaccine). This vaccine is designed as a two series vaccine with the second injection 1-6 months following the initial shot. Local pain and discomfort is significantly higher with this second generation vaccine. Other systemic symptoms such as fever, upset stomach and muscle pain occur.
With Shingrix vaccination, there has also been documented an increase rate of Guillain-Barré syndrome. This is an auto-immune attack of the motor nerves resulting in potentially life-threatening muscle weakness in an ascending fashion. This condition is managed with plasmapheresis (filtering the blood of auto-antibodies) and symptom management, including potentially hospitalization and ventilator support if the diaphragm undergoes paralysis. This is rare but it is a real syndrome. Most patient will recover BUT it can result in significant disability for months and sometimes permanent localized limb weakness/paresis. I recall as a medical student, a faculty doctor dependent upon a cane following getting this illness.
The study reported is from January of this year and published in The Annals of Internal Medicine, a lead Internal Medicine medical journal. It is a good study with a huge patient year data experience. It was designed as a real world effectiveness study asking if the initial trial showing over 90% protection holds up over time. The study also answered a few other questions that needed sorting. One of the issues was if one shot was enough. A second issue is for persons who didn’t get the vaccine in the 6 month window, did a later second injection still work?
My older patients will remember that when this vaccine rolled out there was a big marketing mistake. The company didn’t anticipate wholesale endorsement by the Medicare age and up group. This was the initial targeted group due to the natural history of higher risk of shingles as we move past the 5th decade of life. The result of that market miscalculation was a large number of patients couldn’t get the second shot in the 6 month window. From the study’s date 32% of the subjects didn’t get the vaccine in the 6 month window. 90% got the second shot by one year.
Bullet Points From This Study
Nearly 2 million persons studied. 7.6 million person-years of follow-up. Follow-up period was 4 years.
There were 45,330 new cases defined by clinical diagnosis combined with anti-viral medication prescribed. 94% of the cases were in the unvaccinated group. The unvaccinated group was much larger in size.
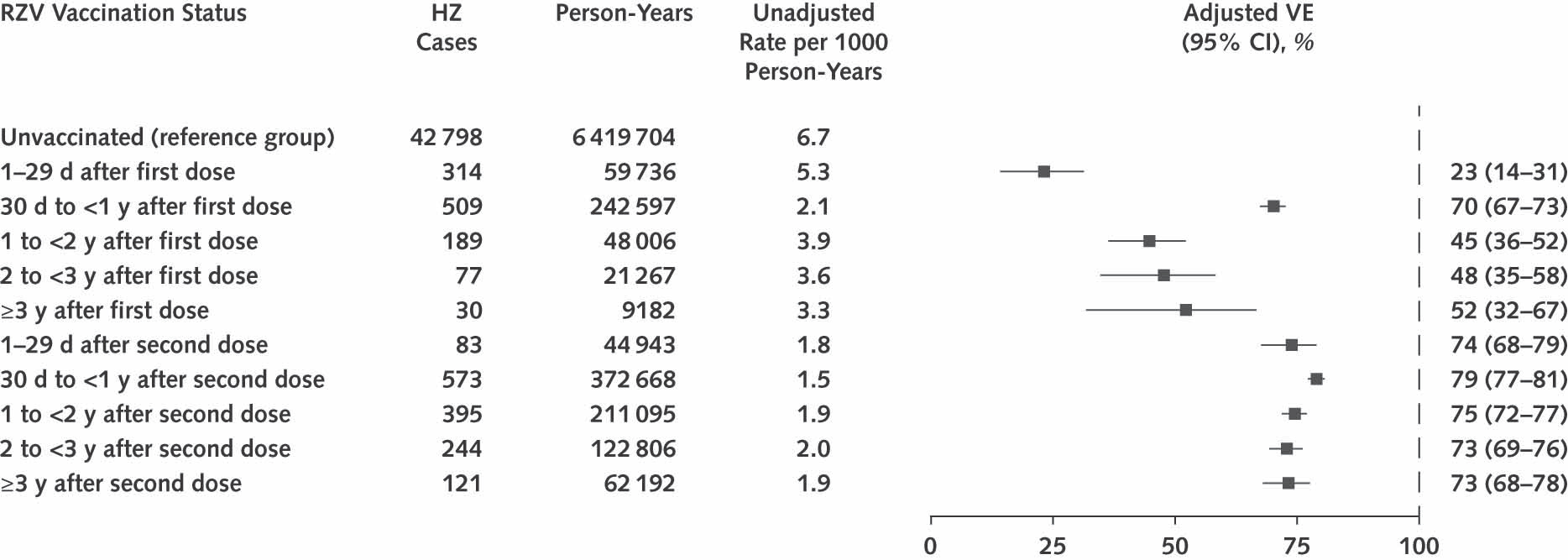
Incidence of clinical shingles was 6.7 per 1000 person-year in the unvaccinated and 1.7 per 1000 person-years in the fully vaccinated. Fully vaccinated means two injections provided.
In partially vaccinated (one shot patients), the efficacy was 64% and 76% for the fully vaccinated.
The effectiveness didn’t change much at 4 years compared to initial 6 months.
Having had steroids prior to vaccination did lower the “take rate” 65% vs 77%
Getting the second dose past one year was not significantly less effective than within the recommended 6 months or at 6-12 months.
Doctor Kordonowy’s Distillation From This Study

The lifetime risk of clinical shingles is moderately high at one in three.
There can be significant morbidity and there can be real disability from this disease.
The newer Shingrix works better than the original shingles adult vaccine and seems to hold up over time. The article references 3 other longer term studies that have found the same results.
Getting a late second shot appears to add efficacy similar to getting the injection as initially studied. This question has come up several times in my practice.
IF patients get diagnosed and treated early morbidity is significantly reduced.
Very risk adverse, working persons will likely find hesitancy for this vaccine due to the package insert acknowledged relationship of clinical Guillain-Barré syndrome. Disability from work would be life-changing.
Person’s with autoimmune illnesses getting immunosuppression therapies will have to weigh the theoretic concerns of stimulating the immune system with vaccination vs increased risk of active shingles and herpes vaccine with immunosuppressive therapy. In my view, patients and treating physicians have mixed and sometimes opposing thoughts on this issue.
So Enough Of The Medical Stuff, Lets’ Discuss Hospital Consolidation and Physician Unionization.
One of my fellow doctor colleagues sent me a Perspective/Editorial article recently published in the New England Journal of Medicine. Dr. Kevin Shulman M.D., and Barak Richman J.D., Ph.D point out that there has been a sea change in physician-practice structures.
They report that since 2012 we have gone from 5.6% of physicians were directly employed by hospitals and a further 23% were partially hospital employed and as of 2022, 52% of physicians were hospital employed and a further 22% were employed by other corporate entities.
The above quote is an astounding set of figures. To me it is literally mind-blowing!
The authors point out that this transition from professional independence to employment and corporate affiliation is an argument for the practicality of unionization for physicians. They go on to point out a rational for why unionization may make sense for physicians. They also do conclude that it is too early to tell if this is how the profession will find itself in response to the present dynamics.
For me I think if doctors unionize, they have admitted the defeat of the profession of medicine. I think such a result basically means an acceptance of the socialization of health care and the end of professional autonomy. If we aren’t independent professionals, we won’t be able to treat ourselves with mutual respect and we certainly won’t be in a position to advocate for individual patients. As a union, we will find ourselves selecting a few likely administrative lapdog physicians arguing for more time off, more perks, average and even pay for mediocre and average patient results in exchange. That will truly be a sad day for patients.
I hope our younger generation of physicians who have been conditioned these past 12 years to accept being the lackey for corporate gurus and hospital protocols snap out of the hypnosis and return to gaining back their self respect and get back to their Hippocratic oath.
In the oath, the physician pledges to prescribe only beneficial treatments, according to his abilities and judgment; to refrain from causing harm or hurt; and to live an exemplary personal and professional life.
I think you are already there. Don't forget COVID, where doctors were sure (or at least claiming) that drugs like HCQ were dangerous despite their safe use for 60+ years, and that the vaccine was wonderful despite its obvious shortcomings. I know its difficult to stand up to pressure given the time and effort it takes to get the degree and establish a practice and I think that most folks are not willing to risk that so they are like sheep following the proverbial Judas goat.
As to patients, unfortunately you are dealing with largely uneducated people who don't know when they are being told foolish things or are being given a bad diagnosis. They will 'stand on line' if they have to or they will populate the emergency rooms. I am sorry but I don't see things changing for the better in the near future, but keep up the good fight
Thanks for your info…I should have listened to you when I was 50. It’s not lollipops and rainbows!